
IAR Overview
Full implementation of the National Intake, Assessment & Referral Tool
The Intake Assessment and Referral (IAR) Tool is a national tool used across all PHNs and State services. It was designed to assist service providers to assess client need and then determine level of care and most appropriate referral path or service.
The IAR is for:
- General Practitioners (GP) and other clinicians seeking to make referrals
- Intake teams including commissioned providers responsible for undertaking initial assessments and/or recommending the level of care required
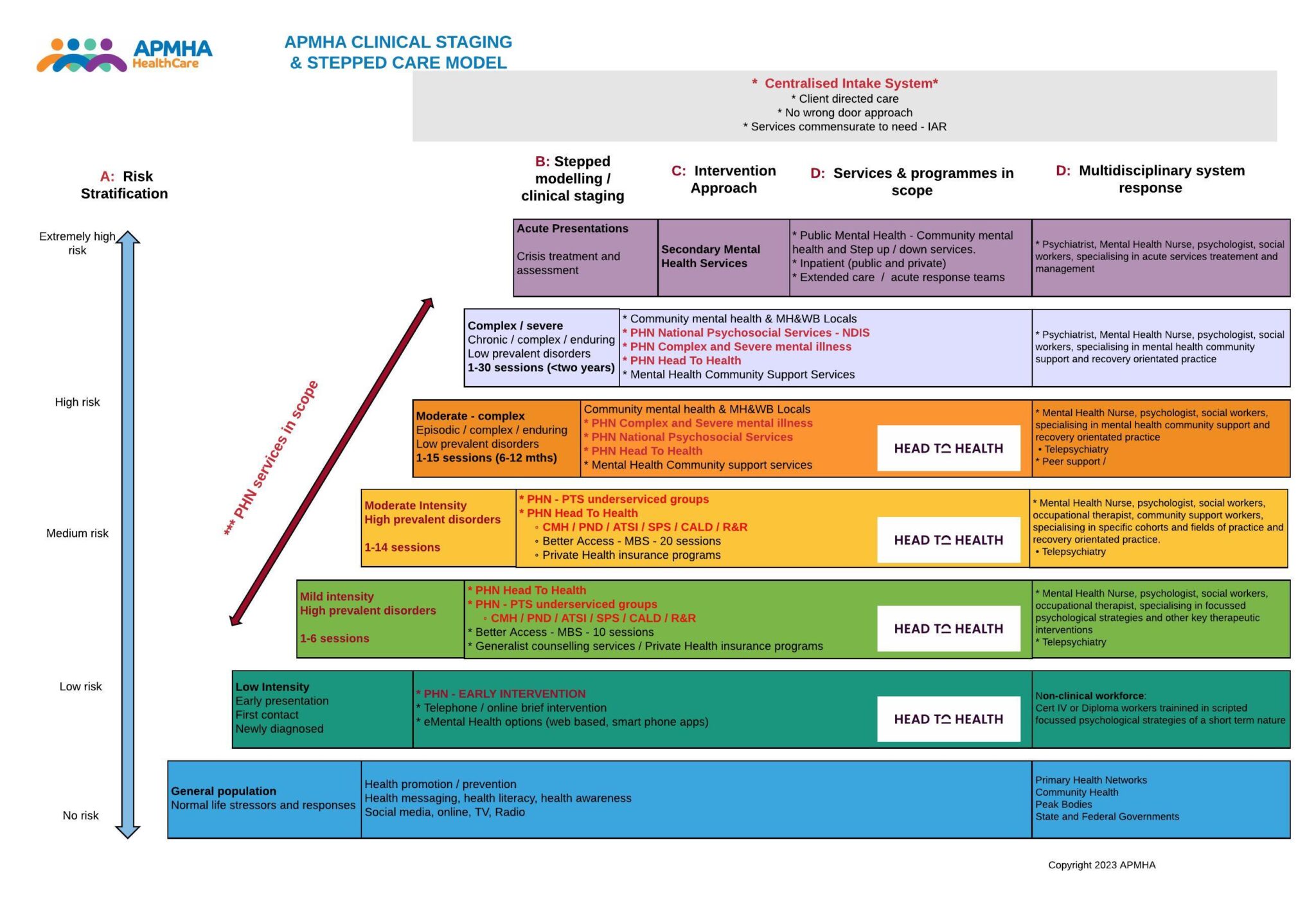
Our Stepped Model
APMHA HealthCare has developed a Service Delivery Framework to reflect a Stepped Mental Health Model of care which sets out the strategic direction of the Company. In APMHAs stepped care model we:
- ensure clients receive care commensurate to need, this being determined by the IAR assessment on intake or at their first appointment.
- ensure person centered care which targets the needs of the individual and recognises that needs may change at any time
- work in strong collaboration and partnership with general practice, carers, and other stakeholders
- focus on the client’s trajectory for their determined recovery
- facilitates seamless transition of clients up / down a stepped mental continuum whilst maintaining continuity of service provision.
Services we deliver under Stepped Care

IAR to Intake, Assessment and Referral via APMHA Intake Team
- Central & Eastern Sydney PHN
- Murray PHN
- North Western Melbourne PHN
- South Western Sydney PHN
Low intensity Mental Health Services (dark blue)
Level 2 – level of care need
Telehealth service provision with linkage to online services.
- Murray PHN

Psychological Therapy Services (Light Green and Dark Green)
Level 3 Level of care need
- Murray PHN
- Central & Eastern Sydney PHN
- North Western Melbourne PHN
- Western Victoria PHN
Severe and Persistent Mental Illness and Care Coordination
Level 4 (light purple and dark purple)
- South Western Sydney PHN
- Murray PHN
Vulnerable Cohorts we support
A focus on vulnerable cohorts which includes specifically trained clinicians providing:
Child Mental Health Services & groups
Refers to children who are aged between 0-12 years, who have, or are at risk of developing a behavioural / emotional / mental health disorder.
These include:
- A child assessed as having definite or substantial signs and symptoms of an emerging mental health disorder, where this causes significant dysfunction in everyday life and/or
- A child at risk of developing a mental health disorder, where the child shows a number of signs and symptoms ( whether that be social, emotional or behavioural) and where the child’s developmental pathway is disrupted by their mental health clinician.
APMHA delivers Child focused mental health services to most regions, with Central and Eastern Sydney and Murray regions being the highest referral rates. In the Murray region we deliver both individual and group options to these clients.
Our Child clinicians are credentialed to provide services to children and are highly experienced.



Youth
Youth services refer to people aged between 13-25 who may benefit from psychological support. While Headspace also offers this service, APMHA often works with clients from this cohort who are transitioning out of Headspace or may not wish to join the Headspace service. APMHA provides services to young people across most service regions, with Central and Eastern Sydney having the highest referral rates for this cohort.
Aboriginal and Torres Strait Islander people
Through APMHA Services, Aboriginal and Torres Strait Islander people are able to access mental health services that are integrated, culturally appropriate and safe. Aboriginal and Torres Strait Islander services are designed to holistically meet the mental health and healing needs of this population group and are delivered by clinicians with additional training in Cultural Awareness. APMHA provides mental health support to Aboriginal and Torres Strait Islanders across all regions and prioritises training opportunities to all workforce.
Our clinicians are credentialed to provide services to Aboriginal & Torres Strait Islander communities and are highly experienced.
Culturally and Linguistically Diverse people
Many PHN Needs Assessments recoginise that access to psychological therapy can be impacted by low English proficiency, cultural stigma and limited support networks. Due to this, interpreter services are available throughout all APMHA Services and culturally appropriate clinicians are made available in all APMHA programs. APMHA also priortises training in this area, ensuring training is always available to clinicians.
Perinatal
Many of our PTS/PSS services prioritise this cohort as the national perinatal depression initiative (2013) recognised the need to improve prevention and early detection of antenatal and postnatal depression. APMHA continues to support this initiative through the Central and Eastern Sydney region and is currently working towards a pilot service in the Murray region.
Suicide Prevention Services
This service provides priority access for Individuals who have attempted, or are at risk of, suicide or self-harm or who have suicidal ideation and are already being managed in the primary health care setting. While APMHA works with the Suicide Prevention Services in most regions, this is not acute care and tends to focus more on reducing Suicide Ideation.
Residential Aged Care Facility
This service allows residents of aged care facilities to access the psychological support available to others in the community. APMHA clinicians travel out to Residential Aged Care Facilities across Murray, Western Victoria and North Western Melbourne regions.
Employee Assistance Program (EAP)
Our tailored Employees Assistance Program (EAP) is a boutique service, offering organisation employees specialist counselling and wellbeing support. It encompasses training, counselling and critical incident and wellbeing support. EAP is delivered by APMHAs a highly proficient, experienced and specialised accredited mental health workforce, which includes psychologists, mental health nurses, mental health occupational therapists and mental health social workers.


Special Projects
SWAP – Findings from the Staff Wellbeing Access Program
The SWAP Team would like to formally thank NWMPHN and the project staff, for the identification of need and subsequent funding to support the RACF workforce. The collaboration and close working relationship developed between NWMPHN as the funding body, and the APMHA SWAP Team, allowed for flexibility, innovation, and a more nuanced response for the RACF workforce’s identified growing mental health needs. This collaboration also provided real-time in depth understanding of what the RACF workforce were / are facing day to day. The SWAP team was permitted to tailor the program as each variant emerged and subsequently, the mental health needs of the workforce increased. Our clinical expertise informed the methodology of the SWAP program design, which led to careful development of a mental health program that is as flexible in the ever-changing climate of the COVID 19 virus.
COVID-19 was a new frontier for mental health service delivery. Developing a flexible response that would meet the varying landscape, has been challenging. However, we endeavored to be innovative to meet each need as it evolved to ensure the most appropriate supportive program for the RACF Workforce.
The RACF workforce was and continues to be significantly impacted by the COVID 19 Pandemic.
The impact of COVID 19 (Alpha) on the RACF workforce was wide ranging and the SWAP team were confronted with an environment that was unique to a typical disaster mental health response. The issues faced by RACFs included the outcomes from the Royal Commission into Aged Care, the ongoing negative media focus and coverage, the quick adaptation of RACFs to their work practices, roles and intensity that a mostly non-clinical workforce had to respond to through infection control measures, PPE, lockdowns, resident isolation and residents’ safety, whilst managing increasing frustration and anxiety with families. Although the SWAP Team employed a disaster response methodology – what became apparent is that this disaster was not going to end any time soon (unlike a bushfire).
What was (and still is) clear, is that RACFs are in a continual phase of “acute response” and not able to focus on recovery. Each time there is a glimmer of movement out of the response phase, another wave and variant emerged, or fresh outbreak in their respective RACF, plunging them back to acute response phase. Some 2.5 years on, response is ongoing.

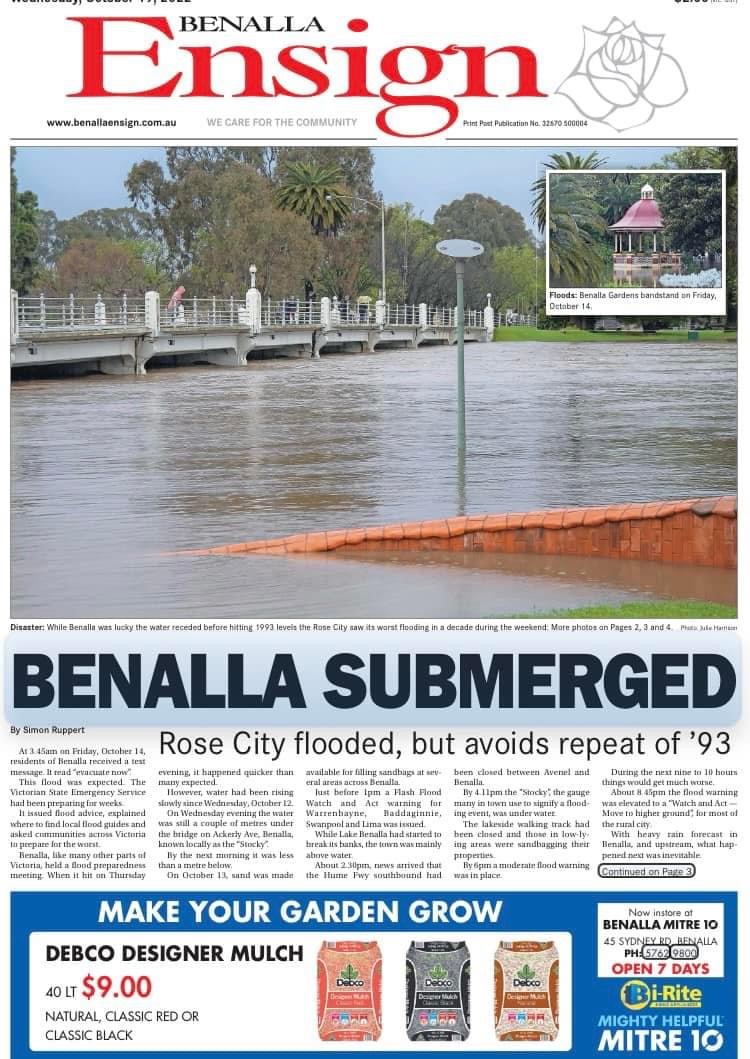
Flood response & recovery
APMHA were one of the first responders to meet the mental health needs of people impacted by the floods in the Shepparton and surrounding areas, with our staff attending local community hubs, relief centres, aged care facilities, as well as out reaching to homes, as soon as it was safe to do so.
All clients engaged with APMHA at that time were contacted to assess for flood impact and ascertain any need for support.





Wellness Hub
APMHA received funding through APNA and Murray to pilot a Nurse Run clinic, focusing on clients with more complex mental health conditions and medications who were at risk of metabolic syndrome.



Significant physical and mental health improvements were noted and comprehensive collaborative management plans were developed with each client’s GP for ongoing care arrangements.